
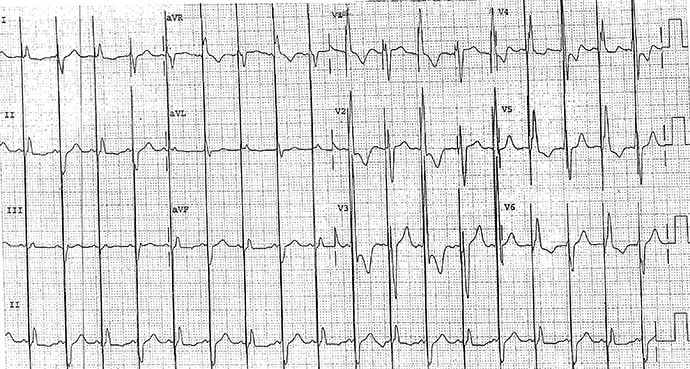
A 78-year-old man with a history of heart failure presents for routine follow-up 1 week after insertion of a pacemaker. As part of the evaluation, a 12-lead ECG is obtained.
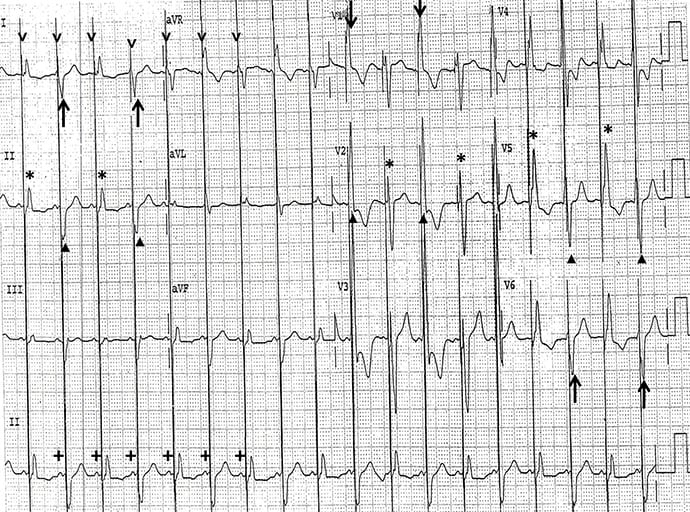
The correct diagnosis is biventricular pacemaker with intermittent loss of left ventricular capture, atrial-sensed and ventricular-paced (Figure 2).
Discussion
There is a regular rhythm at a rate of 110 beats/min. P waves occur before each QRS complex (+) with a stable PR interval (0.12 sec). The P waves are positive in leads I, II, aVF, and V4-V6. This is a sinus tachycardia.
A pacemaker stimulus occurs before each QRS complex (˅). This is considered atrial-sensed ventricular pacing or P wave–synchronous ventricular pacing. However, there are beat-to-beat changes in the QRS complex morphology.
The odd numbered QRS complexes (*) have a normal morphology, axis, and duration (0.08 sec). This suggests that the complexes are not caused by the pacemaker stimulus, but rather are native QRS complexes. The presence of a ventricular pacemaker stimulus before these complexes means that they are pseudofused — in other words, the pacemaker has delivered a stimulus that does not capture because the atrioventricular (AV) delay of the pacemaker is the same as the intrinsic PR interval. Hence, conduction through the AV node His-Purkinje system causes activation of the ventricle at the same time as the pacemaker stimulus.
The even-numbered QRS complexes (▲) have a QS morphology in leads I and V5-V6 (↑) and a tall R wave in lead V1 (↓). This QRS complex morphology is consistent with initial stimulation from the left ventricle and is a result of biventricular pacing. Therefore, there is intermittent failure of left ventricular capture.
Philip Podrid, MD, is an electrophysiologist, a professor of medicine and pharmacology at Boston University School of Medicine, and a lecturer in medicine at Harvard Medical School. Although retired from clinical practice, he continues to teach clinical cardiology and especially ECGs to medical students, house staff, and cardiology fellows at many major teaching hospitals in Massachusetts. In his limited free time he enjoys photography, music, and reading.